
Page 154 - Journal of Special Operations Medicine - Spring 2017
P. 154
An Ongoing Series
Ultrasound-Guided Airway Management
in the Austere Setting
Justin C. Rapp, 18D; Katarzyna (Kasia) Hampton, MD
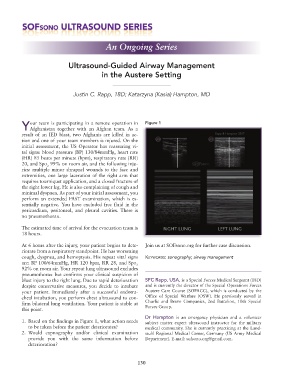
our team is participating in a remote operation in Figure 1
YAfghanistan together with an Afghan team. As a
result of an IED blast, two Afghanis are killed in ac-
tion and one of your team members is injured. On the
initial assessment, the US Operator has reassuring vi-
tal signs: blood pressure (BP) 130/84mmHg, heart rate
(HR) 85 beats per minute (bpm), respiratory rate (RR)
20, and Spo 99% on room air, and the following inju-
2
ries: multiple minor shrapnel wounds to the face and
extremities, one large laceration of the right arm that
requires tourniquet application, and a closed fracture of
the right lower leg. He is also complaining of cough and
minimal dyspnea. As part of your initial assessment, you
perform an extended FAST examination, which is es-
sentially negative. You have excluded free fluid in the
pericardium, peritoneal, and pleural cavities. There is
no pneumothorax.
The estimated time of arrival for the evacuation team is
18 hours.
At 6 hours after the injury, your patient begins to dete- Join us at SOFsono.org for further case discussion.
riorate from a respiratory standpoint. He has worsening
cough, dyspnea, and hemoptysis. His repeat vital signs Keywords: sonography; airway management
are: BP 100/64mmHg, HR 120 bpm, RR 28, and Spo
2
92% on room air. Your repeat lung ultrasound excludes
pneumothorax but confirms your clinical suspicion of
blast injury to the right lung. Due to rapid deterioration SFC Rapp, USA, is a Special Forces Medical Sergeant (18D)
despite conservative measures, you decide to intubate and is currently the director of the Special Operations Forces
your patient. Immediately after a successful endotra- Austere Care Course (SOFACC), which is conducted by the
cheal intubation, you perform chest ultrasound to con- Office of Special Warfare (OSW). He previously served in
firm bilateral lung ventilation. Your patient is stable at Charlie and Bravo Companies, 2nd Battalion, 10th Special
Forces Group.
this point.
Dr Hampton is an emergency physician and a volunteer
1. Based on the findings in Figure 1, what action needs subject matter expert ultrasound instructor for the military
to be taken before the patient deteriorates? medical community. She is currently practicing at the Land-
2. Would capnography and/or clinical examination stuhl Regional Medical Center, Germany (US Army Medical
provide you with the same information before Department). E-mail: sofsono.org@gmail.com.
deterioration?
130