
Page 100 - Journal of Special Operations Medicine - Fall 2016
P. 100
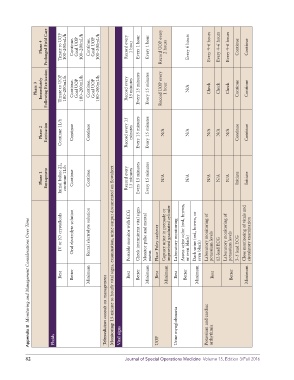
Phase 4 Prolonged Field Care Titrate to UOP 100–200mL/h Continue. Goal UOP 100–200mL/h Continue. Goal UOP 100–200mL/h Record every 1 hour Every 1 hour Every 1 hour Record UOP every 2 hours Every 6 hours Every 4–6 hours Every 4–6 hours Every 4–6 hours Continue Continue Consider fasciotomy. If no improvement, place two tourniquets side by side and proximal to the injury. Amputation anticipated Refer to Pain/ sedation CPG
Phase 3 Immediately Following Extrication Titrate to UOP 100–200mL/h Continue. Goal UOP 100–200mL/h Continue. Goal UOP 100–200mL/h Record every 15 minutes Every 15 minutes Every 15 minutes Record UOP every 1 hour N/A Check Check Check Continue Continue Monitor; repeat as required Monitor; repeat as required Fasciotomy: only if qualified medical personnel or teleconsultation available Cool limb (evaporative or environmental cooling
Phase 2 Extrication Continue 1L/h Continue Continue Record every 15 minutes Every 15 minutes Every 15 minutes N/A N/A N/A N/A N/A Continue Continue N/A N/A N/A N/A N/A N/A N/A — loosening tourniquet. Per TCCC Ertapenem, 1g IV/day (1g, 10mL saline or sterile water) Cefazolin, 2g IV every 6 to 8 hours; clindamycin (300–450mg by mouth three times daily or 600mg IV every 8 hours); or moxifloxacin (400mg/day; IV or by mouth) —
Phase 1 Entrapment Initial bolus: 2L, continue 1L/h Continue Continue Record every 15 minutes Every 15 minutes Every 15 minutes N/A N/A N/A N/A N/A Initiate Initiate N/A N/A N/A N/A N/A N/A N/A — If entrapment time >2 hours, consider tourniquet. Place two tourniquets side by side and proximal to the injury Per TCCC — N/A, not applicable; UOP, urine output. *6 Ps: Pain persisting despite adequate analgesia is most important symptom,
IV or IO crystalloids Oral electrolyte solution Rectal electrolyte solution Portable monitor with ECG Check intermittent vital signs Monitor pulse and mental Place Foley catheter Capture urine in premade or improvised graduated cylinder Laboratory monitoring Assess urine color (red, brown, or even black) Dark urine (red, brown, or even black) Laboratory monitoring of potassium levels 12-lead ECG Laboratory monitoring of potassium levels 3–5 l
Appendix B Monitoring and Management Considerations Over Time
Best Better Minimum Monitoring: 15-minute to hourly vital signs, examination, urine output documented on flowsheet Best Better Minimum status Best Minimum Best Better Minimum Best Better Minimum Treatments for Hyperkalemia (>5.5mEq/L) or Cardiac Arrhythmia Best Better Minimum • 6 Ps* Best Minimum Best Best Better Minimum status
Telemedicine: consult on management Potassium and cardiac Calcium gluconate (10%) Insulin (regular) and D50 Albuterol (2.5mg/3mL vial) Sodium polystyrene sulfonate Calcium gluconate 10% Alternate: calcium chloride 10% Insulin (regular) and D50 Any individual or combination Management of Injured Extremity Extremity compartment (for crush management) (for irreversible injury)
Fluids Vital signs UOP Urine myoglobinuria arrhythmia (Kayexalate) of above, as available syndrome Tourniquet Tourniquet Pain Infection control Antibiotics
82 Journal of Special Operations Medicine Volume 15, Edition 3/Fall 2016