
Page 46 - Journal of Special Operations Medicine - Spring 2016
P. 46
same model replaced the damaged device; the present tensioned to compress the underlying tissue. Further spi-
testing intended that each device tested was structur- ral wrapping distally, down the limb, with the running end
ally and functionally normal. Devices were examined allowed 1.5–3 inches of tissue width to be compressed.
throughout testing for structural and functional integ- After compression was complete, a cleat allowed tension
rity Data were collected February to August, 2014. of the running end to be held by the tourniquet itself so
the user’s hands were freed. At the time of assessment,
The RATS is a commercially developed tactical tourni- the RATS was not in the US Food and Drug Administra-
quet. It has a wrap design with a long, flexible, cloth- tion (FDA) registry of medical devices, but subsequently
covered, rubber-like band; it is oval in cross-section it was registered after our suggestion to the maker.
(4mm × 12.5mm) (Figure 1). The running end is routed
through the other end’s loop, and the running end is The TMT is a tactical tourniquet initially developed by
the US Army. It has a strap-and-windlass design, with a
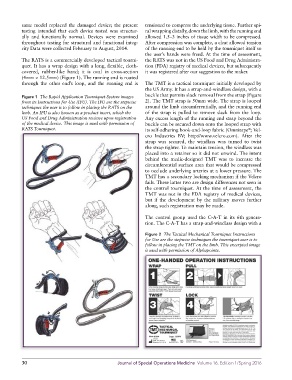
Figure 1 The Rapid Application Tourniquet System images buckle that permits slack removal from the strap (Figure
from its Instructions for Use (IFU). The IFU are the stepwise 2). The TMT strap is 50mm wide. The strap is looped
techniques the user is to follow in placing the RATS on the around the limb circumferentially, and the running end
limb. An IFU is also known as a product insert, which the of the strap is pulled to remove slack from the loop.
US Food and Drug Administration reviews upon registration Any excess length of the running end strap beyond the
of the medical device. This image is used with permission of buckle can be secured down onto the looped strap with
RATS Tourniquet. its self-adhering hook-and-loop fabric (Omnitape ; Vel-
®
cro Industries BV; http://www.velcro.com). After the
strap was secured, the windlass was turned to twist
the strap tighter. To maintain tension, the windlass was
placed into a retainer so it did not unwind. The intent
behind the medic-designed TMT was to increase the
circumferential surface area that would be compressed
to occlude underlying arteries at a lower pressure. The
TMT has a secondary locking mechanism if the Velcro
fails. These latter two are design differences not seen in
the control tourniquet. At the time of assessment, the
TMT was not in the FDA registry of medical devices,
but if the development by the military moves further
along, such registration may be made.
The control group used the C-A-T in its 6th genera-
tion. The C-A-T has a strap-and-windlass design with a
Figure 2 The Tactical Mechanical Tourniquet Instructions
for Use are the stepwise techniques the tourniquet user is to
follow in placing the TMT on the limb. This excerpted image
is used with permission of Alphapointe.
30 Journal of Special Operations Medicine Volume 16, Edition 1/Spring 2016