
Page 69 - Journal of Special Operations Medicine - Fall 2015
P. 69
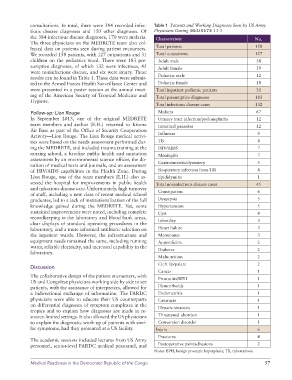
consultations. In total, there were 384 recorded infec- Table 1 Patients and Working Diagnoses Seen by US Army
tious disease diagnoses and 150 other diagnoses. Of Physicians During MEDRETE 13-3
the 384 infectious disease diagnoses, 170 were malaria. Characteristic No.
The three physicians on the MEDRETE team also col-
lected data on patients seen during patient encounters. Total patients 158
We recorded 158 patients, with 127 outpatients and 31 Total outpatients 127
children on the pediatrics ward. There were 183 pre- Adult male 38
sumptive diagnoses, of which 132 were infectious, 45 Adult female 59
were noninfectious disease, and six were injury. These
results can be found in Table 1. These data were submit- Pediatric male 12
ted to the Armed Forces Health Surveillance Center and Pediatric female 18
were presented in a poster session at the annual meet- Total inpatient pediatric patients 31
ing of the American Society of Tropical Medicine and Total presumptive diagnoses 183
Hygiene.
Total infectious disease cases 132
Follow-up: Lion Rouge Malaria 67
In September 2013, one of the original MEDRETE Urinary tract infection/pyelonephritis 12
team members and author (E.H.) returned to Kitona Intestinal parasites 12
Air Base as part of the Office of Security Cooperation Influenza 9
Activity—Lion Rouge. The Lion Rouge medical activi-
ties were based on the needs assessment performed dur- TB 8
ing the MEDRETE, and included trauma training at the HIV/AIDS 7
nursing school, a baseline public health and sanitation Meningitis 7
assessment by an environmental science officer, the do- Gastroenteritis/dysentery 5
nation of medical texts and journals, and an assessment
of HIV/AIDS capabilities in the Health Zone. During Respiratory infection (non-TB) 4
Lion Rouge, one of the team members (E.H.) also as- Epididymitis 1
sessed the hospital for improvements in public health Total noninfectious disease cases 45
and infectious disease care. Unfortunately, high turnover Constipation 6
of staff, including a new class of recent medical school
graduates, led to a lack of institutionalization of the full Dyspepsia 5
knowledge gained during the MEDRETE. Yet, some Hypertension 5
sustained improvements were noted, including complete Cyst 4
recordkeeping in the laboratory and blood bank areas, Infertility 3
clear displays of standard operating procedures in the
laboratory, and a more informed antibiotic selection on Heart failure 3
the inpatient wards. However, the infrastructure and Menopause 3
equipment needs remained the same, including running Appendicitis 2
water, reliable electricity, and increased capability in the Diabetes 2
laboratory.
Malnutrition 2
Cleft lip/palate 2
Discussion
Cancer 1
The collaborative design of the patient encounters, with Prostatitis/BPH 1
US and Congolese physicians working side by side to see
patients, with the assistance of interpreters, allowed for Hemorrhoids 1
a bidirectional exchange of information. The FARDC Endometritis 1
physicians were able to educate their US counterparts Cataracts 1
on differential diagnoses of symptom complexes in the Hepatic steatosis 1
tropics and to explain how diagnoses are made in re-
source-limited settings. It also allowed the US physicians Threatened abortion 1
to explain the diagnostic work-up of patients with simi- Conversion disorder 1
lar symptoms, had they presented at a US facility. Injury 6
Fractures 4
The academic sessions included lectures from US Army
personnel, senior-level FARDC medical personnel, and Postoperative pain/adhesions 2
Notes: BPH, benign prostatic hyperplasia; TB, tuberculosis.
Medical Readiness in the Democratic Republic of the Congo 57