
Page 91 - Journal of Special Operations Medicine - Summer 2015
P. 91
event into context. However, the provider should adhere to Although patients may present with symptoms that appear
basic questions, as probing or unnecessary questions can ex- to be consistent with PTSD, providers should realize that
acerbate symptoms. traumatic brain injury (TBI) symptoms overlap with PTSD
symptoms. In our clinical experience, patients who have ex-
1. PCL-M score ≥50, positive CAPS, or PCL-5 score ≥40? perienced a moderate to severe TBI may not directly benefit
(Note: If score is not achieved, but patient has significant from SGB. However, patients with both a TBI and concomi-
PTSD symptoms, clinician should still consider treating.) tant PTSD may benefit from SGB treatment. If a patient has
10
2. Confirm duration of symptom clusters: a history of mild TBI with full recovery, they should be consid-
• Intrusion ered for treatment and may be included in study populations.
• Avoidance
• Negative alterations in cognitions and mood
• Alterations in arousal and reactivity Key Points for Treatment
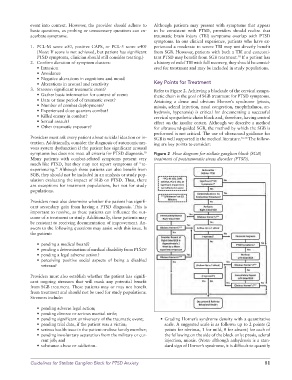
3. Stressor: significant traumatic event? Refer to Figure 2. Achieving a blockade of the cervical sympa-
• Gather basic information for context of event: thetic chain is the goal of SGB treatment for PTSD symptoms.
• Date or time period of traumatic event? Attaining a dense and obvious Horner’s syndrome (ptosis,
• Number of combat deployments? miosis, scleral injection, nasal congestion, enophthalmos, an-
• Experienced close quarters combat? hydrosis, hyperemia) is critical for documenting a successful
• Killed enemy in combat? cervical sympathetic chain block and, therefore, having central
• Sexual assault? effect on the insular cortex. Although we describe a method
• Other traumatic exposure? for ultrasound-guided SGB, the method by which the SGB is
performed is not critical. The use of ultrasound guidance for
Providers must ask every patient about suicidal ideation or in- SGB is well supported in the medical literature. 16-18 The follow-
tention. Additionally, consider the diagnosis of autonomic ner- ing are key points to consider:
vous system dysfunction if the patient has significant arousal
symptoms but does not meet all criteria for PTSD diagnosis. Figure 2 Flow diagram for stellate ganglion block (SGB)
10
Many patients with combat-related symptoms present very treatment of posttraumatic stress disorder (PTSD).
much like PTSD, but they may not report symptoms of “re-
experiencing.” Although these patients can also benefit from
SGB, they should not be included in an analysis or study pop-
ulation evaluating the impact of SGB on PTSD. Thus, there
are exceptions for treatment populations, but not for study
populations.
Providers must also determine whether the patient has signifi-
cant secondary gain from having a PTSD diagnosis. This is
important to resolve, as these patients can influence the out-
come of a treatment or study. Additionally, these patients may
be resistant to receiving documentation of improvement. An-
swers to the following questions may assist with this issue. Is
the patient:
• pending a medical board?
• pending a determination of medical disability from PTSD?
• pending a legal adverse action?
• perceiving positive social aspects of being a disabled
veteran?
Providers must also establish whether the patient has signifi-
cant ongoing stressors that will mask any potential benefit
from SGB treatment. These patients may or may not benefit
from treatment and should not be used for study populations.
Stressors include:
• pending adverse legal action;
• pending divorce or serious marital strife;
• pending significant anniversary of the traumatic event; • Grading Horner’s syndrome density with a quantitative
• pending trial date, if the patient was a victim; scale. A suggested scale is as follows: up to 2 points (2
• serious health issue in the patient or close family member; points for obvious, 1 for mild, 0 for absent) for each of
• pending involuntary separation from the military or cur- the following on the side of the block only: ptosis, scleral
rent job; and injection, miosis. (Note: although anhydrosis is a stan-
• substance abuse or addiction. dard sign of Horner’s syndrome, it is difficult to quantify
Guidelines for Stellate Ganglion Block for PTSD Anxiety 81