
Page 59 - Journal of Special Operations Medicine - Summer 2015
P. 59
Rochester in Minnesota). Combined, they employ 400 Tourniquet
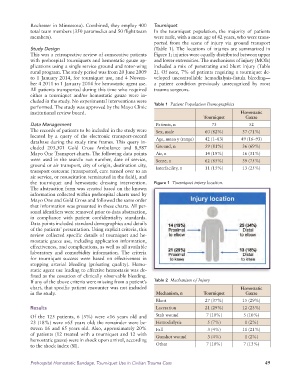
total team members (350 paramedics and 50 flight team In the tourniquet population, the majority of patients
members). were male, with a mean age of 42 years, who were trans-
ported from the scene of injury via ground transport
Study Design (Table 1). The locations of injuries are summarized in
This was a retrospective review of consecutive patients Figure 1; injuries were equally distributed between upper
with prehospital tourniquets and hemostatic gauze ap- and lower extremities. The mechanisms of injury (MOIs)
plications using a single service ground and rotor-wing included a mix of penetrating and blunt injury (Table
rural program. The study period was from 20 June 2009 2). Of note, 7% of patients requiring a tourniquet de-
to 1 January 2014, for tourniquet use, and 4 Novem- veloped uncontrollable hemodialysis-fistula bleeding—
ber 4 2011 to 1 January 2014 for hemostatic agent use. a patient condition previously unrecognized by most
All patients transported during this time who required trauma surgeons.
either a tourniquet and/or hemostatic gauze were in-
cluded in the study. No experimental interventions were Table 1 Patient Population Demographics
performed. The study was approved by the Mayo Clinic
institutional review board. Hemostatic
Tourniquet Gauze
Data Management Patients, n 73 52
The records of patients to be included in the study were Sex, male 60 (82%) 37 (71%)
located by a query of the electronic transport-record Age, mean y (range) 42 (1–83) 49 (16–93)
data base during the study time frames. This query in-
cluded 203,301 Gold Cross Ambulance and 8,987 Ground, n 59 (81%) 36 (69%)
Mayo One Transport charts. The following data points Air, n 14 (19%) 16 (31%)
were used in the search: run number, date of service, Scene, n 62 (85%) 39 (75%)
ground or air transport, city of origin, destination city, Interfacility, n 11 (15%) 13 (25%)
transport outcome (transported, care turned over to an
air service, or resuscitation terminated in the field), and
the tourniquet and hemostatic dressing intervention. Figure 1 Tourniquet injury location.
The abstraction form was created based on the known
information collected within prehospital charts used by
Mayo One and Gold Cross and followed the same order
that information was presented in these charts. All per-
sonal identifiers were removed prior to data abstraction,
in compliance with patient confidentiality standards.
Data points included standard demographics and details
of the patients’ presentation. Using explicit criteria, this
review collected specific details of tourniquet and he-
mostatic gauze use, including application information,
effectiveness, and complications, as well as all available
laboratory and comorbidity information. The criteria
for tourniquet success were based on effectiveness in
stopping arterial bleeding (pulsating quality). Hemo-
static agent use leading to effective hemostasis was de-
fined as the cessation of clinically observable bleeding.
If any of the above criteria were missing from a patient’s Table 2 Mechanism of Injury
chart, that specific patient encounter was not included Hemostatic
in the study. Mechanism, n Tourniquet Gauze
Blunt 27 (37%) 15 (29%)
Results Laceration 21 (29%) 12 (23%)
Of the 125 patients, 6 (5%) were <16 years old and Stab wound 7 (10%) 5 (10%)
23 (18%) were >65 years old; the remainder were be- Hemodialysis 5 (7%) 1 (2%)
tween 16 and 65 years old. Also, approximately 20% Fall 3 (4%) 11 (21%)
of patients (12 treated with a tourniquet and 12 with Gunshot wound 3 (4%) 1 (2%)
hemostatic gauze) were in shock upon arrival, according
to the shock index (SI). Other 7 (10%) 7 (13%)
Prehospital Hemostatic Bandage, Tourniquet Use in Civilian Trauma Care 49