
Page 97 - Journal of Special Operations Medicine - Spring 2015
P. 97
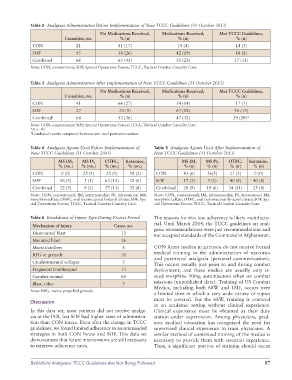
Table 2 Analgesia Administration Before Implementation of New TCCC Guidelines (31 October 2013)
No Medications Received, Medications Received, Met TCCC Guidelines,
Casualties, no. % (n) % (n) % (n)
CON 21 81 (17) 19 (4) 14 (3)
SOF 45 58 (26) 42 (19) 18 (8)
Combined 66 65 (43) 35 (23) 17 (11)
Note: CON, conventional; SOF, Special Operations Forces; TCCC, Tactical Combat Casualty Care.
Table 3 Analgesia Administration After Implementation of New TCCC Guidelines (31 October 2013)
No Medications Received, Medications Received, Met TCCC Guidelines,
Casualties, no. % (n) % (n) % (n)
CON 41 66 (27) 34 (14) 17 (7)
SOF 27 33 (9) 67 (18) 48 (13)
Combined † 68 53 (36) 47 (32) 29 (20)*
Note: CON, conventional; SOF, Special Operations Forces; TCCC, Tactical Combat Casualty Care.
*p < .10.
† Combined results compared between pre and postintervention.
Table 4 Analgesia Agents Used Before Implementation of Table 5 Analgesia Agents Used After Implementation of
New TCCC Guidelines (31 October 2013) New TCCC Guidelines (31 October 2013)
MS IM, MS IV, OTFC, Ketamine, MS IM, MS IV, OTFC, Ketamine,
% (no.) % (no.) % (no.) % (no.) % (n) % (n) % (n) % (n)
CON 0 (0) 25 (1) 25 (1) 50 (2) CON 43 (6) 36(5) 21 (3) 0 (0)
SOF 26 (5) 5 (1) 63 (12) 32 (6) SOF 17 (3) 5 (1) 40 (8) 40 (8)
Combined 22 (5) 9 (2) 57 (13) 35 (8) Combined 28 (9) 19 (6) 34 (11) 25 (8)
Note: CON, conventional; IM, intramuscular; IV, intravenous; MS, Note: CON, conventional; IM, intramuscular; IV, intravenous; MS,
morphine sulfate; OTFC, oral transmucosal fentanyl citrate; SOF, Spe morphine sulfate; OTFC, oral transmucosal fentanyl citrate; SOF, Spe
cial Operations Forces; TCCC, Tactical Combat Casualty Care. cial Operations Forces; TCCC, Tactical Combat Casualty Care.
Table 6 Breakdown of Injury Type During Project Period The reasons for this low adherence is likely multifacto
Mechanism of Injury Cases, no. rial. Until March 2014, the TCCC guidelines on anal
Dismounted blast 13 gesia recommendations were just recommendations and
not accepted standards of the Command in Afghanistan.
Mounted blast 16
Mortar/artillery 8 CON Army medics in garrison do not receive formal
RPG or grenade 16 medical training in the administration of narcotics
Crush/structural collapse 3 and parenteral analgesia (personal communication).
This occurs usually just prior to and during combat
Fragmentation/shrapnel 15 deployment, and these medics are usually only is
Gunshot wound 60 sued morphine 10mg autoinjectors when on combat
Blast, other 3 missions (unpublished data). Training of US Combat
Note: RPG, rocketpropelled grenade. Medics, including both 68W and 18D, occurs over
a limited time in which a very wide variety of topics
must be covered. For the 68W, training is centered
Discussion
in an academic setting without clinical experience.
In this data set, most patients did not receive analge Clinical experience must be obtained at their duty
sia at the POI, but SOF had higher rates of administra station under supervision. Among physicians, grad
tion than CON forces. Even after the change in TCCC uate medical education has recognized the need for
guidelines, we found limited adherence to recommended supervised clinical experience to train physicians. A
strategies in both CON forces and SOF. This data set similar method of continued training of the medics is
demonstrates that future interventions are still necessary necessary to provide them with essential experience.
to improve adherence rates. Thus, a significant portion of training should occur
Battlefield Analgesia: TCCC Guidelines Are Not Being Followed 87