
Page 41 - Journal of Special Operations Medicine - Summer 2014
P. 41
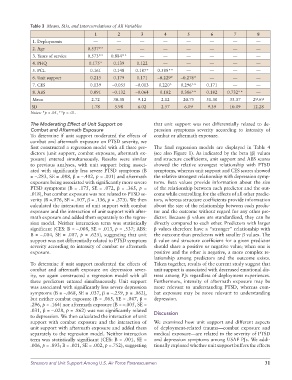
Table 3 Means, SDs, and Intercorrelations of All Variables
1 2 3 4 5 6 7 8
1. Deployments — — — — — — — —
2. Age 0.537** — — — — — — —
3. Years of service 0.573** 0.884** — — — — — —
4. PHQ 0.175* 0.139 0.122 — — — — —
5. PCL 0.161 0.148 0.187* 0.589** — — — —
6. Unit support 0.215 0.179 0.171 –0.229* –0.276* — — —
7. CES 0.139 –0.055 –0.013 0.220* 0.296** 0.171 — —
8. ABS 0.091 –0.132 –0.064 0.182 0.386** 0.182 0.732** —
Mean 2.72 30.38 9.12 2.12 20.75 51.30 33.37 29.69
SD 1.78 5.98 6.02 2.57 6.09 9.39 10.09 12.28
Notes: *p < .05, **p < .01.
The Moderating Effect of Unit Support on that unit support was not differentially related to de-
Combat and Aftermath Exposure pression symptoms severity according to intensity of
To determine if unit support moderated the effects of combat or aftermath exposure.
combat and aftermath exposure on PTSD severity, we
first constructed a regression model with all three pre- The final regression models are displayed in Table 4
dictors (unit support, combat exposure, aftermath ex- (see also Figure 1). As indicated by the beta (β) values
posure) entered simultaneously. Results were similar and structure coefficients, unit support and ABS scores
to previous analyses, with unit support being associ- showed the relative strongest relationship with PTSD
ated with significantly less severe PTSD symptoms (B symptoms, whereas unit support and CES scores showed
= –.283, SE = .088, β = –.402, p < .001) and aftermath the relative strongest relationship with depression symp-
exposure being associated with significantly more severe toms. Beta values provide information about the size
PTSD symptoms (B = .175, SE = .072, β = .365, p = of the relationship between each predictor and the out-
.018), but combat exposure was not related to PTSD se- come while controlling for the effects of all other predic-
verity (B =.076, SE = .107, β = .136, p = .373). We then tors, whereas structure coefficients provide information
calculated the interaction of unit support with combat about the size of the relationship between each predic-
exposure and the interaction of unit support with after- tor and the outcome without regard for any other pre-
math exposure and added them separately to the regres- dictor. Because β values are standardized, they can be
sion model. Neither interaction term was statistically directly compared to each other. Predictors with larger
significant (CES: B = –.008, SE = .013, p = .537; ABS: β values therefore have a “stronger” relationship with
B = –.004, SE = .007, p = .625), suggesting that unit the outcome than predictors with smaller β values. The
support was not differentially related to PTSD symptom β value and structure coefficient for a given predictor
severity according to intensity of combat or aftermath should share a positive or negative value; when one is
exposure. positive and the other is negative, a more complex re-
lationship among predictors and the outcome exists.
To determine if unit support moderated the effects of Taken together, results of the current study suggest that
combat and aftermath exposure on depression sever- unit support is associated with decreased emotional dis-
ity, we again constructed a regression model with all tress among PJs regardless of deployment experiences.
three predictors entered simultaneously. Unit support Furthermore, intensity of aftermath exposure may be
was associated with significantly less severe depression more relevant to understanding PTSD, whereas com-
symptoms (B = –.068, SE = .037, β = –.259, p = .062), bat exposure may be more relevant to understanding
but neither combat exposure (B = .065, SE = .047, β = depression.
.296, p = .164) nor aftermath exposure (B = –.005, SE =
.031, β = –.028, p = .862) was not significantly related
to depression. We then calculated the interaction of unit Discussion
support with combat exposure and the interaction of We examined how unit support and different aspects
unit support with aftermath exposure and added them of deployment-related trauma—combat exposure and
separately to the regression model. Neither interaction medical exposure—are related to the severity of PTSD
term was statistically significant (CES: B = .001, SE = and depression symptoms among USAF PJs. We addi-
.006, p = .893; B = .001, SE = .002, p =.752), suggesting tionally explored whether unit support buffers the effects
Stressors and Unit Support Among U.S. Air Force Pararescuemen 31