
Page 115 - JSOM Spring 2023
P. 115
An updated clinical practice guideline. Am Surg. 2022; 88(4): 27. April MD, Bridwell RE, Jones J, et al. Descriptive analysis of ca-
674–679. sualties rapidly returned to the fight after injury: Reverse triage
23. Chapman BC, Herbert B, Rodil M, et al. RibScore: A novel radio- implications for large scale combat operations. Med J (Ft Sam
graphic score based on fracture pattern that predicts pneumonia, Houst Tex). 2022;Per 22-04-05-06(Per 22-04-05-06):3–9.
respiratory failure, and tracheostomy. J Trauma Acute Care Surg. 28. April MD, Stednick PJ, Christian NB. A descriptive analysis of na-
2016;80(1):95–101. tional casualties sustained at the Joint Readiness Training Center:
24. Hardin KS, Leasia KN, Haenel J, et al. The Sequential Clinical Implications for health service support during large-scale combat
Assessment of Respiratory Function (SCARF) score: A dynamic operations. Med J (Ft Sam Houst Tex). 2021(Pb 8-21-04/05/06):
pulmonary physiologic score that predicts adverse outcomes in 3–8.
critically ill rib fracture patients. J Trauma Acute Care Surg. 2019; 29. Garamone J. Leaders update Special Ops vision, strategy. 11
87(6):1260–1268. April 2022. https://www.defense.gov/News/News-Stories/Article/
25. Timofte I, Diaz-Abad M, Alghanim F, et al. Spirometry testing for Article/2995785/leaders-update-special-ops-vision-strategy/. Ac-
extracorporeal membrane oxygenation (ECMO) bridge to trans- cessed 27 January 2023.
plant patients. Respir Med Case Rep. 2022;36:101577. 30. Schroen J. What the new vision for the US Special Operations gets
26. Tran D, Lim M, Vogrin S, Jayaram L. Point of care portable spi- right—and wrong. 18 April 2022. https://mwi.usma.edu/what-
rometry in the diagnosis and treatment of inpatients with chronic the-new-vision-for-us-special-operations-gets-right-and-wrong/.
obstructive pulmonary disease. Lung. 2020;198(1):143–150. Accessed 27 January 2023.
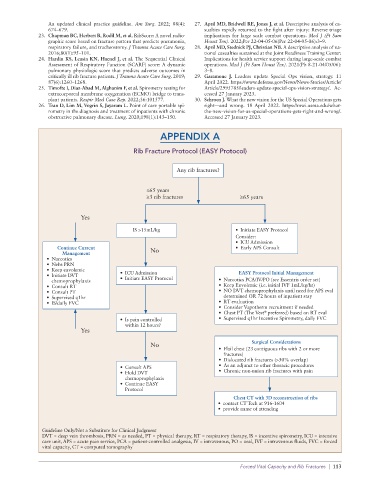
APPENDIX A
Rib Fracture Protocol (EASY Protocol)
Any rib fractures?
≤65 years
≥3 rib fractures ≥65 years
Yes
IS >15mL/kg • Initiate EASY Protocol
Consider:
• ICU Admission
Continue Current No • Early APS Consult
Management
• Narcotics
• Nebs PRN
• Keep euvolemic
• Initiate DVT • ICU Admission EASY Protocol Initial Management
chemoprophylaxis • Initiate EASY Protocol • Narcotics PCA/IV/PO (see Essentris order set)
• Consult RT • Keep Euvolemic (i.e. initial IVF 1mL/kg/hr)
• Consult PT • NO DVT chemoprophylaxis until need for APS eval
• Supervised q1hr determined OR 72 hours of inpatient stay
• IS/daily FVC • RT evaluation
• Consider Vapotherm recruitment if needed
• Chest PT (The Vest preferred) based on RT eval
®
• Is pain controlled • Supervised q1hr Incentive Spirometry, daily FVC
within 12 hours?
Yes
No Surgical Considerations
• Flail chest (23 contiguous ribs with 2 or more
fractures)
• Dislocated rib fractures (>50% overlap)
• Consult APS • As an adjunct to other thoracic procedures
• Hold DVT • Chronic non-union rib fractures with pain
chemoprophylaxis
• Continue EASY
Protocol
Chest CT with 3D reconstruction of ribs
• contact CT Tech at 916-1604
• provide name of attending
Guideline Only/Not a Substitute for Clinical Judgment
DVT = deep vein thrombosis, PRN = as needed, PT = physical therapy, RT = respiratory therapy, IS = incentive spirometry, ICU = intensive
care unit, APS = acute pain service, PCA = patient-controlled analgesia, IV = intravenous, PO = oral, IVF = intravenous fluids, FVC = forced
vital capacity, CT = computed tomography
Forced Vital Capacity and Rib Fractures | 113