
Page 296 - 2023 SMOG Digital
P. 296
FORMS
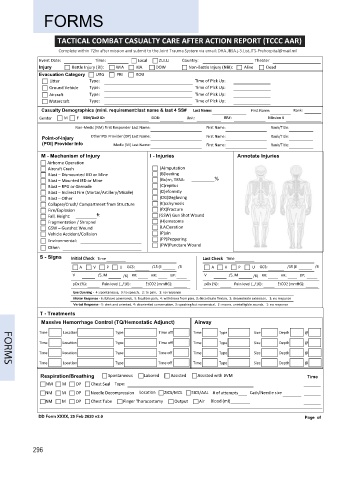
TACTICAL COMBAT CASUALTY CARE AFTER ACTION REPORT (TCCC AAR)
Complete within 72hr after mission and submit to the Joint Trauma System via email: DHA.JBSA.j-3.List.JTS-Prehospital@mail.mil
Event Date: Time: Local ZULU Country: Theater
Injury Battle Injury (BI): WIA KIA DOW Non-Battle Injury (NBI): Alive Dead
Evacuation Category URG PRI ROU
Litter Type: Time of Pick Up:
Ground Vehicle Type: Time of Pick Up:
Aircraft Type: Time of Pick Up:
Watercraft Type: Time of Pick Up:
Casualty Demographics (mini. requirement:last name & last 4 SS# Last Name: First Name: Rank:
Gender M F SSN/DoD ID: DOB: Unit: BR#: Mission #
Non-Medic (NM) First Responder Last Name: First Name: Rank/Title:
Point-of-Injury Other POI Provider (OP) Last Name: First Name: Rank/Title:
(POI) Provider Info Medic (M) Last Name: First Name: Rank/Title:
M - Mechanism of Injury I - Injuries Annotate Injuries
Airborne Operation
Aircraft Crash (A)mputation
Blast – Dismounted IED or Mine (B)leeding
Blast – Mounted IED or Mine (Bu)rn, TBSA: %
Blast – RPG or Grenade (C)repitus
Blast – Indirect Fire (Mortar/Artillery/Missile) (D)eformity
Blast – Other (DG)Degloving
Collapse/Crush/ Compartment from Structure (E)cchymosis
Fire/Explosion (FX)Fracture
Fall, Height: ft (GSW) Gun Shot Wound
Fragmentation / Shrapnel (H)ematoma
GSW – Gunshot Wound (LAC)eration
Vehicle Accident/Collision (P)ain
Environmental: (PP)Peppering
Other: (PW)Puncture Wound
S - Signs Initial Check Last Check
A V P U GCS: /15 (E /4 A V P U GCS: /15 (E /4
V /5, M /6) RR: HR: BP: V /5, M /6) RR: HR: BP:
pOx (%): Pain level (_/10): EtCO2 (mmHG): pOx (%): Pain level (_/10): EtCO2 (mmHG):
Eye Opening - 4: spontaneous, 3: to speech, 2: to pain, 1: no response
Motor Response - 6: follows commands, 5: localizes pain, 4: withdraws from pain, 3: decorticate flexion, 2: decerebrate extension, 1: no response
Verbal Response - 5: alert and oriented, 4: disoriented conversation, 3: speaking but nonsensical, 2: moans, unintelligible sounds, 1: no response
T - Treatments
Massive Hemorrhage Control (TQ/Hemostatic Adjunct) Airway
Time Location Type Time off Time Type Size Depth @
Time Location Type Time off Time Type Size Depth @
Time Location Type Time off Time Type Size Depth @
Time Location Type Time off Time Type Size Depth @
Respiration/Breathing Spontaneous Labored Assisted Assisted with BVM Time
NM M OP Chest Seal Type:
NM M OP Needle Decompression Location 2ICS/MCL 5ICS/AAL # of attempts Cath/Needle size
NM M OP Chest Tube Finger Thoracostomy Output Air Blood (ml)
DD Form XXXX, 25 Feb 2020 v2.0 Page of
296