
Page 257 - 2023 SMOG Digital
P. 257
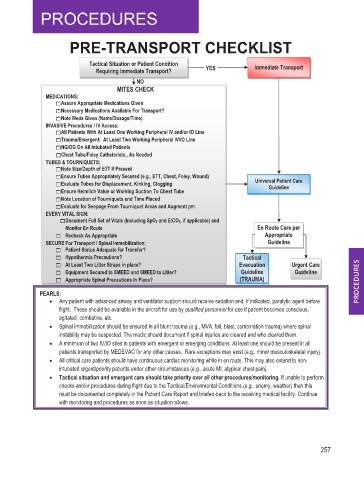
PRE-TRANSPORT CHECKLIST
Tactical Situation or Patient Condition Immediate Transport
Requiring Immediate Transport? YES
NO
MITES CHECK
MEDICATIONS:
Assure Appropriate Medications Given
Necessary Medications Available For Transport?
Note Meds Given (Name/Dosage/Time)
INVASIVE Procedures / IV Access:
All Patients With At Least One Working Peripheral IV and/or IO Line
Trauma/Emergent: At Least Two Working Peripheral IV/IO Line
NG/OG On All Intubated Patients
Chest Tube/Foley Catheter/etc., As Needed
TUBES & TOURNIQUETS:
Note Size/Depth of ETT if Present
Ensure Tubes Appropriately Secured (e.g., ETT, Chest, Foley, Wound)
Evaluate Tubes for Displacement, Kinking, Clogging Universal Patient Care
Guideline
Ensure Heimlich Value or Working Suction To Chest Tube
Note Location of Tourniquets and Time Placed
Evaluate for Seepage From Tourniquet Areas and Augment prn r n
p
EVERY VITAL SIGN:
t
p
Document Full Set of Vitals (Including SpO2 and EtCO2, if applicable) and
Monitor En Route En Route Care per
Recheck As Appropriate Appropriate
SECURE For Transport / Spinal Immobilization: Guideline
Patient Status Adequate for Transfer?
Hypothermia Precautions? Tactical
At Least Two Litter Straps in place? Evacuation Urgent Care
Equipment Secured to SMEED and SMEED to Litter? Guideline Guideline
Appropriate Spinal Precautions in Place? (TRAUMA)
PEARLS:
• Any patient with advanced airway and ventilator support should receive sedation and, if indicated, paralytic agent before
flight. These should be available in the aircraft for use by qualified personnel for use if patient becomes conscious,
agitated, combative, etc.
• Spinal immobilization should be ensured in all blunt trauma (e.g., MVA, fall, blast, combination trauma) where spinal
instability may be suspected. The medic should document if spinal injuries are cleared and who cleared them.
• A minimum of two IV/IO sites in patients with emergent or emerging conditions. At least one should be present in all
patients transported by MEDEVAC for any other causes. Rare exceptions may exist (e.g., minor musculoskeletal injury).
• All critical care patients should have continuous cardiac monitoring while in en route. This may also extend to non-
intubated urgent/priority patients under other circumstances (e.g., acute MI, atypical chest pain).
• Tactical situation and emergent care should take priority over all other procedures/monitoring. If unable to perform
checks and/or procedures during flight due to the Tactical/Environmental Conditions (e.g., enemy, weather) then this
must be documented completely in the Patient Care Report and briefed-back to the receiving medical facility. Continue
with monitoring and procedures as soon as situation allows.
257