
Page 288 - PJ MED OPS Handbook 8th Ed
P. 288
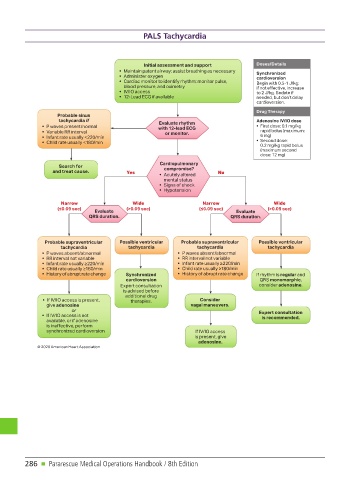
PALS Tachycardia
Pediatric Tachycardia With a Pulse Algorithm
Initial assessment and support Doses/Details
• Maintain patent airway; assist breathing as necessary
Synchronized
• Administer oxygen
cardioversion
• Cardiac monitor to identify rhythm; monitor pulse,
Begin with 0.5-1 J/kg;
blood pressure, and oximetry if not effective, increase
• IV/IO access to 2 J/kg. Sedate if
• 12-Lead ECG if available needed, but don’t delay
cardioversion.
Drug Therapy
Probable sinus
tachycardia if Adenosine IV/IO dose
Evaluate rhythm
• P waves present/normal • First dose: 0.1 mg/kg
with 12-lead ECG
• Variable RR interval rapid bolus (maximum:
or monitor.
• Infant rate usually <220/min 6 mg)
• Second dose:
• Child rate usually <180/min
0.2 mg/kg rapid bolus
(maximum second
dose: 12 mg)
Cardiopulmonary
Search for
compromise?
and treat cause. Yes No
• Acutely altered
mental status
• Signs of shock
• Hypotension
Narrow Wide Narrow Wide
(≤0.09 sec) (>0.09 sec) (≤0.09 sec) (>0.09 sec)
Evaluate Evaluate
QRS duration. QRS duration.
Probable supraventricular Possible ventricular Probable supraventricular Possible ventricular
tachycardia tachycardia tachycardia tachycardia
• P waves absent/abnormal • P waves absent/abnormal
• RR interval not variable • RR interval not variable
• Infant rate usually ≥220/min • Infant rate usually ≥220/min
• Child rate usually ≥180/min • Child rate usually ≥180/min
• History of abrupt rate change Synchronized • History of abrupt rate change If rhythm is regular and
cardioversion QRS monomorphic,
Expert consultation consider adenosine.
is advised before
additional drug
• If IV/IO access is present, therapies. Consider
give adenosine vagal maneuvers.
or
Expert consultation
• If IV/IO access is not
is recommended.
available, or if adenosine
is ineffective, perform
synchronized cardioversion If IV/IO access
is present, give
adenosine.
© 2020 American Heart Association
286 n Pararescue Medical Operations Handbook / 8th Edition