
Page 117 - PJ MED OPS Handbook 8th Ed
P. 117
Epistaxis
SPECIAL CONSIDERATIONS:
1. Common at high altitude and in desert environments due to mucosal drying.
2. May be anterior or posterior.
3. Posterior epistaxis may be difficult to stop and may cause respiratory distress due to blood
flowing into the airway. This type of epistaxis is uncommon in young healthy adults. It is
more commonly seen in older, hypertensive patients.
Signs and Symptoms:
1. Nosebleed
2. Often previous history of nosebleeds
Management:
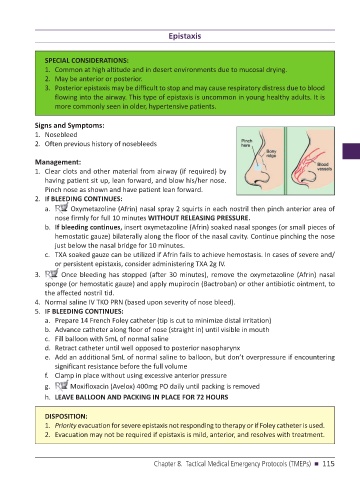
1. Clear clots and other material from airway (if required) by
having patient sit up, lean forward, and blow his/her nose.
Pinch nose as shown and have patient lean forward.
2. If BLEEDING CONTINUES:
a. Oxymetazoline (Afrin) nasal spray 2 squirts in each nostril then pinch anterior area of
nose firmly for full 10 minutes WITHOUT RELEASING PRESSURE.
b. If bleeding continues, insert oxymetazoline (Afrin) soaked nasal sponges (or small pieces of
hemostatic gauze) bilaterally along the floor of the nasal cavity. Continue pinching the nose
just below the nasal bridge for 10 minutes.
c. TXA soaked gauze can be utilized if Afrin fails to achieve hemostasis. In cases of severe and/
or persistent epistaxis, consider administering TXA 2g IV.
3. Once bleeding has stopped (after 30 minutes), remove the oxymetazoline (Afrin) nasal
sponge (or hemostatic gauze) and apply mupirocin (Bactroban) or other antibiotic ointment, to
the affected nostril tid.
4. Normal saline IV TKO PRN (based upon severity of nose bleed).
5. IF BLEEDING CONTINUES:
a. Prepare 14 French Foley catheter (tip is cut to minimize distal irritation)
b. Advance catheter along floor of nose (straight in) until visible in mouth
c. Fill balloon with 5mL of normal saline
d. Retract catheter until well opposed to posterior nasopharynx
e. Add an additional 5mL of normal saline to balloon, but don’t overpressure if encountering
significant resistance before the full volume
f. Clamp in place without using excessive anterior pressure
g. Moxifloxacin (Avelox) 400mg PO daily until packing is removed
h. LEAVE BALLOON AND PACKING IN PLACE FOR 72 HOURS
DISPOSITION:
1. Priority evacuation for severe epistaxis not responding to therapy or if Foley catheter is used.
2. Evacuation may not be required if epistaxis is mild, anterior, and resolves with treatment.
Chapter 8. Tactical Medical Emergency Protocols (TMEPs) n 115