
Page 126 - JSOM Summer 2022
P. 126
diagnostic resources, only 42% of pediatric sepsis patients with the same temperature is more likely to show signs of
meet the current criteria. When examining a sick child, ap- fatigue or AMS. Additionally, the severity of fever does not
29
pearance is often the first observation to give a “sick or not necessarily correlate to the degree of illness. A child with a
sick” impression. Assessment of capillary refill is arguably fever of 39.5°C (103.1°F) exhibiting an engaged affect is likely
the most important preliminary finding when examining not as acutely ill as a child with a 37.9°C (100.2°F) fever who
initial appearance, as delayed capillary refill is a significant is somnolent and disengaged from their parents. Given these
indicator that a patient is compensating poorly and requires considerations, AMS in the presence of fever should prompt
further assessment and intervention. 2,4,23–26 Delayed capillary clinicians to expedite care.
refill is directly associated with hemodynamic compensation
in the septic patient and should guide treatment. Capillary Further assessment of organ systems is needed to create a firm
refill is associated with lactic acidosis, hypoxemia, decreased differential diagnosis for sepsis in the absence of laboratory
renal function, and cardiac output variability. When assessing support. Renal dysfunction, respiratory dysfunction, and car-
global skin presentation, pallor and mottling are commonly diac dysfunction are all commonly observed in septic children.
observed in later sepsis stages, whereas flushing occurs in ear- Oliguria, especially with dark coloration, is a concerning find-
lier stages. A sick child can present as pale or flushed during ing which should create a high index of suspicion for the pres-
initial assessment. However, cold and mottled skin indicates ence of AKI. 20,22,27 Hypoxia, sustained tachypnea, retractions,
an immediate need for intervention as mottling shows loss of and accessory muscle use are all indicators of acute respiratory
vascular tone and cardiac output simultaneously. 4, 23–26 In ad- dysfunction. 2,27 Hypotension, delayed capillary refill, and sus-
dition to skin appearance, a thorough head-to-toe inspection tained tachycardia are indicators of cardiac dysfunction. 4,16,24,25
of the skin’s surface should be performed. Open wounds are The use of strong clinical assessment skills is paramount when
regular sources of infection which lead to sepsis when left un- in the austere environment, and clinicians should be compre-
treated and may have gone unnoticed or poorly treated due hensive with sick children due to the variety of ways they may
to lack of resources. 1,3,27 If an object is found and suspected compensate.
to be causing the septic response, safely removing it is recom-
28
mended. Rashes, purpura, petechiae, sores, and edema are
also essential findings indicative of an infection that will create Vital Signs
a better clinical picture. In young infants and neonates, assess- Appropriate interpretation of vital signs is essential when as-
ment of the fontanelles is necessary to better assess hydration sessing sick children and given the physiologic differences in
status and a potential concern for the meningeal disease. neonatal and pediatric patients, values that may be normal to
these patients can be concerning when compared to adult vital
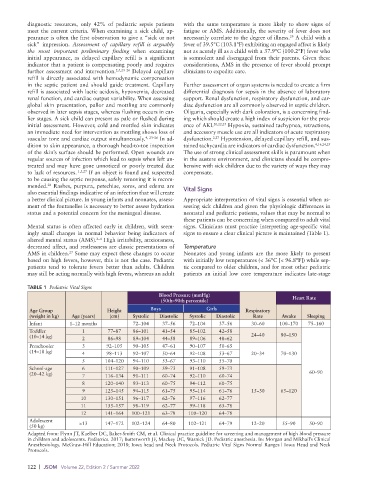
Mental status is often affected early in children, with seem- signs. Clinicians must practice interpreting age-specific vital
ingly small changes in normal behavior being indicators of signs to ensure a clear clinical picture is maintained (Table 1).
2–4
altered mental status (AMS). High irritability, anxiousness,
decreased affect, and restlessness are classic presentations of Temperature
27
AMS in children. Some may expect these changes to occur Neonates and young infants are the more likely to present
based on high fevers, however, this is not the case. Pediatric with initially low temperatures (< 36°C [< 96.8°F]) while sep-
patients tend to tolerate fevers better than adults. Children tic compared to older children, and for most other pediatric
may still be acting normally with high fevers, whereas an adult patients an initial low core temperature indicates late-stage
TABLE 1 Pediatric Vital Signs
Blood Pressure (mmHg)
(50th–90th percentile) Heart Rate
Age Group Height Boys Girls Respiratory
(weight in kg) Age (years) (cm) Systolic Diastolic Systolic Diastolic Rate Awake Sleeping
Infant 1–12 months 72–104 37–56 72–104 37–56 30–60 100–170 75–160
Toddler 1 77–87 86–101 41–54 85–102 42–58
(10–14 kg) 2 86–98 89–104 44–58 89–106 48–62 24–40 80–150
Preschooler 3 92–105 90–105 47–61 90–107 50–65
(14–18 kg) 4 98–113 92–107 50–64 92–108 53–67 20–34 70–130
5 104–120 94–110 53–67 93–110 55–70
School-age 6 111–127 90–109 59–73 91–108 59–73
(20–42 kg) 7 116–134 91–111 60–74 92–110 60–74 60–90
8 120–140 93–113 60–75 94–112 60–75
9 125–145 94–115 61–75 95–114 61–76 15–30 65–120
10 130–151 96–117 62–76 97–116 62–77
11 135–157 98–119 62–77 99–118 63–78
12 141–164 100–121 63–78 100–120 64–78
Adolescent
(50 kg) >13 147–172 102–124 64–80 102–121 64–79 12–20 55–90 50–90
Adapted from: Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure
in children and adolescents. Pediatrics. 2017; Butterworth JF, Mackey DC, Wasnick JD. Pediatric anesthesia. In: Morgan and Mikhail’s Clinical
Anesthesiology. McGraw-Hill Education; 2018; Iowa head and Neck Protocols. Pediatric Vital Signs Normal Ranges | Iowa Head and Neck
Protocols.
122 | JSOM Volume 22, Edition 2 / Summer 2022