
Page 77 - Journal of Special Operations Medicine - Fall 2016
P. 77
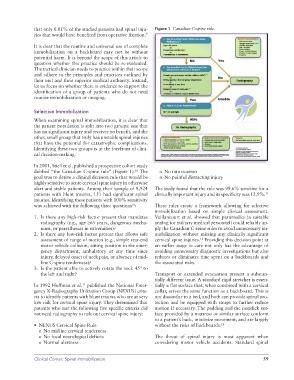
that only 0.01% of the studied patients had spinal inju- Figure 1 Canadian C-spine rule.
ries that would have benefited from operative fixation. 9
It is clear that the routine and universal use of complete
immobilization on a backboard may not be without
potential harm. It is beyond the scope of this article to
question whether this practice should be re-evaluated.
The tactical clinician needs to practice within their scope
and adhere to the principles and practices outlined by
their unit and their superior medical authority. Instead,
let us focus on whether there is evidence to support the
identification of a group of patients who do not need
routine immobilization or imaging.
Selective Immobilization
When examining spinal immobilization, it is clear that
the patient population is split into two groups: one that
has no significant injury and receives no benefit, and the
other, small group that truly has unstable spinal injuries
that have the potential for catastrophic complications.
Identifying these two groups is at the forefront of clini-
cal decision-making.
In 2001, Stiell et al. published a prospective cohort study
dubbed “the Canadian C-spine rule” (Figure 1). The o No intoxication
10
goal was to derive a clinical decision rule that would be o No painful distracting injury
highly sensitive to acute cervical spine injury in otherwise
alert and stable patients. Among their sample of 8,924 The study found that the rule was 99.6% sensitive for a
patients with blunt trauma, 151 had significant spinal clinically important injury and its specificity was 12.9%. 11
injuries. Identifying these patients with 100% sensitivity
was achieved with the following three questions : These rules create a framework allowing for selective
10
immobilization based on simple clinical assessment.
1. Is there any high-risk factor present that mandates Vaillancourt et al. showed that paramedics (a suitable
radiography (e.g., age ≥65 years, dangerous mecha- analog for military medical personnel) could reliably ap-
nism, or paresthesias in extremities)? ply the Canadian C-spine rules to avoid unnecessary im-
2. Is there any low-risk factor present that allows safe mobilization without missing any clinically significant
assessment of range of motion (e.g., simple rear-end cervical spine injuries. Providing this decision point at
12
motor vehicle collision, sitting position in the emer- an earlier stage in care not only has the advantage of
gency department, ambulatory at any time since avoiding unnecessary diagnostic investigations but also
injury, delayed onset of neck pain, or absence of mid- reduces or eliminates time spent on a backboards and
line C-spine tenderness)? the associated risks.
3. Is the patient able to actively rotate the neck 45° to
the left and right? Transport or extended evacuation present a substan-
tially different issue. A standard rigid stretcher is essen-
In 1992 Hoffman et al. published the National Emer- tially a flat surface that, when combined with a cervical
11
gency X-Radiography Utilization Group (NEXUS) crite- collar, serves the same function as a backboard. This is
ria to identify patients with blunt trauma who are at very not dissimilar to a bed, and both can provide spinal pro-
low risk for cervical spine injury. They determined that tection and be equipped with straps to further reduce
patients who met the following five specific criteria did motion if necessary. The padding and the nonslick sur-
not need radiography to rule out cervical spine injury: face provided by a mattress or similar surface conform
to a patient’s back, minimize movement, and are largely
• NEXUS Cervical Spine Rule without the risks of backboards. 13
o No midline cervical tenderness
o No focal neurological deficits The threat of spinal injury is most apparent when
o Normal alertness considering motor vehicle accidents. Standard spinal
Clinical Corner: Spinal Immobilization 59