
Page 16 - Journal of Special Operations Medicine - Summer 2016
P. 16
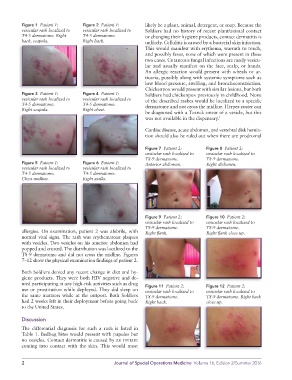
Figure 1 Patient 1: Figure 2 Patient 1: likely be a plant, animal, detergent, or soap. Because the
vesicular rash localized to vesicular rash localized to Soldiers had no history of recent plant/animal contact
T4-5 dermatome. Right T4-5 dermatome. or changing their hygiene products, contact dermatitis is
back, scapula. Right back. unlikely. Cellulitis is caused by a bacterial skin infection.
This would manifest with erythema, warmth to touch,
and possibly fever, none of which were present in these
two cases. Cutaneous fungal infections are rarely vesicu-
lar and usually manifest on the face, scalp, or hands.
An allergic reaction would present with wheals or ur-
ticaria, possibly along with systemic symptoms such as
low blood pressure, swelling, and bronchoconstriction.
Chickenpox would present with similar lesions, but both
Figure 3 Patient 1: Figure 4 Patient 1: Soldiers had chickenpox previously in childhood. None
vesicular rash localized to vesicular rash localized to of the described rashes would be localized to a specific
T4-5 dermatome. T4-5 dermatome. dermatome and not cross the midline. Herpes zoster can
Right scapula. Right chest.
be diagnosed with a Tzanck smear of a vesicle, but this
was not available in the dispensary. 1
Cardiac disease, acute abdomen, and vertebral disk hernia-
tion should also be ruled out when there are prodromal
Figure 7 Patient 2: Figure 8 Patient 2:
vesicular rash localized to vesicular rash localized to
T8-9 dermatome. T8-9 dermatome.
Figure 5 Patient 1: Figure 6 Patient 1: Anterior abdomen. Right abdomen.
vesicular rash localized to vesicular rash localized to
T4-5 dermatome. T4-5 dermatome.
Chest midline. Right axilla.
Figure 9 Patient 2: Figure 10 Patient 2:
vesicular rash localized to vesicular rash localized to
T8-9 dermatome. T8-9 dermatome.
allergies. On examination, patient 2 was afebrile, with Right flank. Right flank close up.
normal vital signs. The rash was erythematous plaques
with vesicles. Two vesicles on his anterior abdomen had
popped and crusted. The distribution was localized to the
T8-9 dermatome and did not cross the midline. Figures
7–12 show the physical examination findings of patient 2.
Both Soldiers denied any recent change in diet and hy-
giene products. They were both HIV negative and de-
nied participating in any high-risk activities such as drug Figure 11 Patient 2: Figure 12 Patient 2:
use or prostitution while deployed. They did sleep on vesicular rash localized to vesicular rash localized to
the same mattress while at the outpost. Both Soldiers T8-9 dermatome. T8-9 dermatome. Right back
had 2 weeks left in their deployment before going back Right back. close up.
to the United States.
Discussion
The differential diagnosis for such a rash is listed in
Table 1. Bedbug bites would present with papules but
no vesicles. Contact dermatitis is caused by an irritant
coming into contact with the skin. This would most
2 Journal of Special Operations Medicine Volume 16, Edition 2/Summer 2016