
Page 60 - Journal of Special Operations Medicine - Fall 2015
P. 60
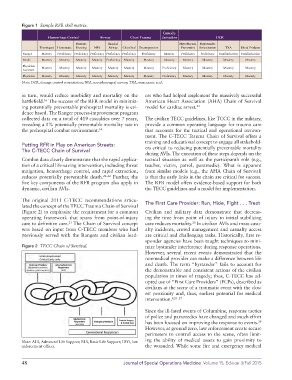
Figure 1 Sample RFR skill matrix.
Casualty
Hemorrhage Control Airway Chest Trauma Extraction DCR
Pressure Surgical Hypothermia Hypotensive
Tourniquet Hemostatic Dressing NPA Airway Chest Seal Decompression Prevention Resuscitation TXA Blood Products
Ranger Mastery Proficiency Proficiency Proficiency Proficiency Proficiency Proficiency Mastery Proficiency Proficiency Familiarization Familiarization
Medic Mastery Mastery Mastery Mastery Proficiency Mastery Mastery Mastery Mastery Mastery Mastery Mastery
Physician Mastery Mastery Mastery Mastery Mastery Mastery Mastery Proficiency Mastery Mastery Mastery Mastery
Assistant
Physician Mastery Mastery Mastery Mastery Mastery Mastery Mastery Proficiency Mastery Mastery Mastery Mastery
Note: DCR, damage control resuscitation; NPA, nasopharyngeal airway; TXA, tranexamic acid.
in turn, would reduce morbidity and mortality on the ers who had helped implement the massively successful
battlefield. The success of the RFR model in minimiz- American Heart Association (AHA) Chain of Survival
16
ing potentially preventable prehospital mortality is evi- model for cardiac arrest. 24
dence based. The Ranger process-improvement program
collected data on a total of 419 casualties over 7 years, The civilian TECC guidelines, like TCCC in the military,
revealing a 0% potentially preventable mortality rate in provide a common operating language for trauma care
the prehospital combat environment. 14 that accounts for the tactical and operational environ-
ment. The C-TECC Trauma Chain of Survival offers a
training and educational concept to engage all stakehold-
Putting RFR in Play on American Streets: ers critical to reducing potentially preventable mortality
The C-TECC Chain of Survival
during AVIs. The execution of these steps depends on the
Combat data clearly demonstrate that the rapid applica- tactical situation as well as the participant’s role (e.g.,
tion of a critical life-saving intervention, including threat teacher, victim, patrol, paramedic). What is apparent
mitigation, hemorrhage control, and rapid extraction, from similar models (e.g., the AHA Chain of Survival)
reduces potentially preventable death. 20–22 Further, the is that the early links in the chain are critical for success.
five key components of the RFR program also apply in The RFR model offers evidence-based support for both
dynamic, civilian AVIs. the TECC guidelines and a model for implementation.
The original 2011 C-TECC recommendations articu- The First Care Provider: Run, Hide, Fight . . . Treat
lated the concept of the TECC Trauma Chain of Survival
(Figure 2) to emphasize the requirement for a common Civilian and military data demonstrate that decreas-
operating framework that spans from point-of-injury ing the time from point of injury to initial stabilizing
care to definitive care. The Chain of Survival concept care reduces mortality. In civilian AVIs and mass casu-
20
23
was based on input from C-TECC members who had alty incidents, crowd management and casualty access
previously served with the Rangers and civilian lead- are critical and challenging tasks. Historically, first re-
sponder agencies have been taught techniques to mini-
Figure 2 TECC Chain of Survival. mize bystander interference during response operations.
However, several recent events demonstrated that the
nonmedical provider can make a difference between life
and death. The term “bystander” fails to account for
the demonstrable and consistent actions of the civilian
population in times of tragedy; thus, C-TECC has ad-
opted use of “First Care Providers” (FCPs), described as
civilians at the scene of a traumatic event with the clos-
est proximity and, thus, earliest potential for medical
intervention. 8,25–27
Since the ill-fated events of Columbine, response tactics
of police and paramedics have changed and much effort
has been focused on improving the response to events.
28
However, at ground zero, law enforcement create secure
perimeters to control access to the scene, often limit-
Note: ALS, Advanced Life Support; BLS, Basic Life Support; LEO, law ing the ability of medical assets to gain proximity to
enforcement officer. the wounded. While some fire and emergency medical
48 Journal of Special Operations Medicine Volume 15, Edition 3/Fall 2015