
Page 52 - JSOM Winter 2023
P. 52
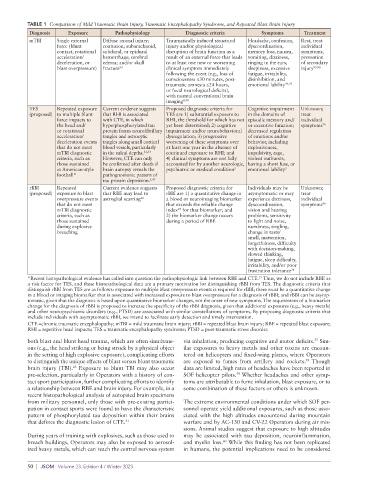
TABLE 1 Comparison of Mild Traumatic Brain Injury, Traumatic Encephalopathy Syndrome, and Repeated Blast Brain Injury
Diagnosis Exposure Pathophysiology Diagnostic criteria Symptoms Treatment
mTBI Single external Diffuse axonal injury; Traumatically induced structural Headache, confusion, Rest, treat
force (blunt contusion; subarachnoid, injury and/or physiological dyscoordination, individual
contact, rotational subdural, or epidural disruption of brain function as a memory loss, nausea, symptoms,
acceleration/ hemorrhage; cerebral result of an external force that leads vomiting, dizziness, prevention
deceleration, or edema; and/or skull to at least one new or worsening ringing in the ears, of secondary
blast overpressure) fracture 93 clinical symptom immediately sleepiness, excessive injury 95,96
following the event (e.g., loss of fatigue, irritability,
consciousness ≤30 minutes, post- disinhibition, and
traumatic amnesia ≤24 hours, emotional lability 94,95
or focal neurological deficits),
with normal conventional brain
imaging 4,94
TES Repeated exposure Current evidence suggests Proposed diagnostic criteria for Cognitive impairment Unknown;
(proposed) to multiple blunt that RHI is associated TES are 1) substantial exposure to in the domains of treat
force impacts to with CTE, in which RHI, the threshold for which has not episodic memory and/ individual
the head and/ hyperphosphorylated tau yet been determined; 2) cognitive or executive function; symptoms 96
or rotational protein forms neurofibrillary impairment and/or neurobehavioral decreased regulation
acceleration/ tangles and astrocytic dysregulation; 3) progressive of emotions and/or
deceleration events tangles along small cortical worsening of these symptoms over behavior, including
that do not meet blood vessels, particularly at least one year in the absence of explosiveness,
mTBI diagnostic in the sulcal depths. 32,33 continued exposure to RHI; and impulsivity, rage,
criteria, such as However, CTE can only 4) clinical symptoms are not fully violent outbursts,
those sustained be confirmed after death if accounted for by another neurologic, having a short fuse, or
in American-style brain autopsy reveals the psychiatric or medical condition emotional lability
5
5
football* pathognomonic pattern of
tau protein deposition. 5,97
rBBI Repeated Current evidence suggests Proposed diagnostic criteria for Individuals may be Unknown;
(proposed) exposure to blast that RBE may lead to rBBI are 1) a quantitative change in asymptomatic or may treat
overpressure events astroglial scarring 26 a blood or neuroimaging biomarker experience dizziness, individual
that do not meet that exceeds the reliable change dyscoordination, symptoms 96
mTBI diagnostic index for that biomarker; and vision and hearing
87
criteria, such as 2) the biomarker change occurs problems, sensitivity
those sustained during a period of RBE to light and noise,
during explosive numbness, tingling,
breaching change in taste/
smell, inattention,
forgetfulness, difficulty
with decision-making,
slowed thinking,
fatigue, sleep difficulty,
irritability, and/or poor
frustration tolerance 36
*Recent histopathological evidence has called into question the pathophysiologic link between RBE and CTE. Thus, we do not include RBE as
31
a risk factor for TES, and these histopathological data are a primary motivation for distinguishing rBBI from TES. The diagnostic criteria that
distinguish rBBI from TES are as follows: exposure to multiple blast overpressure events is required for rBBI; there must be a quantitative change
in a blood or imaging biomarker that is associated with increased exposure to blast overpressure for a diagnosis of rBBI; and rBBI can be asymp-
tomatic, given that the diagnosis is based upon quantitative biomarker changes, not the onset of new symptoms. The requirement of a biomarker
change for the diagnosis of rBBI is proposed to increase the specificity of the rBBI diagnosis, given that additional exposures (e.g., heavy metals)
and other neuropsychiatric disorders (e.g., PTSD) are associated with similar constellations of symptoms. By proposing diagnostic criteria that
include individuals with asymptomatic rBBI, we intend to facilitate early detection and timely intervention.
CTE =chronic traumatic encephalopathy; mTBI = mild traumatic brain injury; rBBI = repeated blast brain injury; RBE = repeated blast exposure;
RHI = repetitive head impacts; TES = traumatic encephalopathy syndrome; PTSD = post-traumatic stress disorder.
both blast and blunt head trauma, which are often simultane- via inhalation, producing cognitive and motor deficits. Sim-
57
ous (e.g., the head striking or being struck by a physical object ilar exposures to heavy metals and other toxins are encoun-
in the setting of high explosive exposure), complicating efforts tered on helicopters and fixed-wing planes, where Operators
58
to distinguish the unique effects of blast versus blunt traumatic are exposed to fumes from artillery and rockets. Though
brain injury (TBI). Exposure to blunt TBI may also occur data are limited, high rates of headaches have been reported in
23
59
pre-selection, particularly in Operators with a history of con- SOF helicopter pilots. Whether headaches and other symp-
tact sport participation, further complicating efforts to identify toms are attributable to fume inhalation, blast exposure, or to
a relationship between RBE and brain injury. For example, in a some combination of these factors or others is unknown.
recent histopathological analysis of autopsied brain specimens
from military personnel, only those with pre-existing partici- The extreme environmental conditions under which SOF per-
pation in contact sports were found to have the characteristic sonnel operate yield additional exposures, such as those asso-
pattern of phosphorylated tau deposition within their brains ciated with the high altitudes encountered during mountain
that defines the diagnostic lesion of CTE. 31 warfare and by AC-130 and CV-22 Operators during air mis-
sions. Animal studies suggest that exposure to high altitudes
During years of training with explosives, such as those used to may be associated with tau deposition, neuroinflammation,
breach buildings, Operators may also be exposed to aerosol- and myelin loss. While this finding has not been replicated
60
ized heavy metals, which can reach the central nervous system in humans, the potential implications need to be considered
50 | JSOM Volume 23, Edition 4 / Winter 2023